 Verinote AI
Verinote AI

An AI medical scribe is software that listens to your patient encounters, transcribes the conversation, and auto-generates a structured clinical note you can review and sign in under 60 seconds. Most platforms cut documentation time per visit by 50–70% and eliminate 1–2 hours of after-hours charting. The trade-off? You’re legally responsible for every word the AI writes, and hallucinations—plausible-sounding text that never happened—are still a real risk.
If you’re averaging 90 minutes of charting after clinic, this guide will show you how AI scribes work, where they fail, and how to pilot one without blowing up your workflow.
What Is an AI Medical Scribe?
An AI medical scribe captures ambient audio during patient visits, uses speech-to-text plus large language models to extract clinical content, and outputs a structured note in SOAP, APSO, or specialty-specific formats. Unlike dictation tools that transcribe verbatim, AI scribes attempt to understand speaker roles, clinical context, and your EHR’s schema so they can auto-populate HPI, ROS, exam findings, assessments, and plans.
Most platforms run in one of three modes:
- Mobile app – records via phone microphone, processes in the cloud, syncs to EHR via API or copy-paste
- Browser plugin – captures system audio during telehealth or ambient listening through laptop mic
- Exam-room hardware – dedicated microphone arrays mounted in clinic rooms
The physician reviews the draft, edits anything wrong, and signs. You’re not saving time if review takes longer than typing the note yourself.
Why Documentation Burden Keeps Growing
I’ve watched documentation time balloon over the last decade. Physicians now spend 1.5–3 hours on charting and inbox work for every hour of face-to-face care, according to JAMA Network studies. Electronic health records were supposed to fix this. They didn’t.
The biggest time sinks:
- Re-typing full histories and exams after every visit
- Copy-pasting labs, meds, imaging results from five different tabs
- Writing similar assessments and plans for the same conditions all day
- Keeping notes compliant for billing codes, quality metrics, and medico-legal defense
AI medical scribes target all of this. Early data from UC San Diego and Stanford shows 50–70% reduction in documentation time when scribes are used consistently. The real win? Less after-hours charting. Burnout studies link late-night documentation to emotional exhaustion more than any other EHR task.
How AI Medical Scribes Actually Work
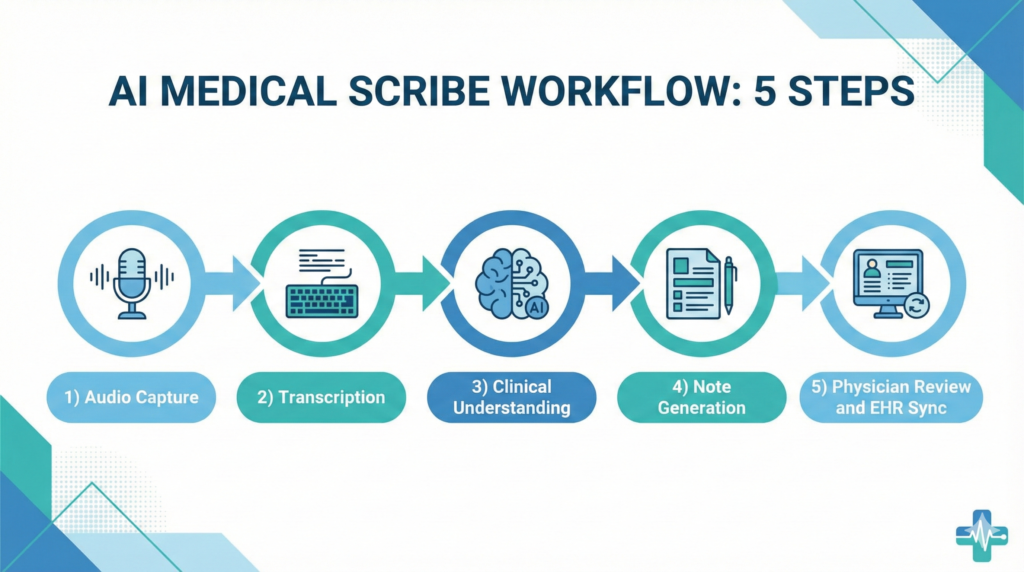
Most platforms follow this pipeline:
1. Audio capture – via mobile app, browser, or exam-room mic. Some integrate directly with Zoom or Doxy.me for telehealth.
2. Speech-to-text – converts conversation to raw transcription. Medical vocabulary models reduce errors on drug names and anatomy.
3. Clinical extraction – AI identifies speakers (doctor vs patient), extracts problems, medications, vitals, physical findings, and decisions using LLMs trained on millions of clinical notes.
4. Note generation – maps extracted data into your EHR’s template. SOAP for primary care. APSO for specialists. Custom formats for hospitalists or ED docs.
5. Physician review – you edit, accept, or reject sections. This step is non-negotiable. The AI will hallucinate. You need to catch it.
6. EHR sync – final note pushes into Epic, Cerner, or Athena via FHIR API, HL7 interface, or manual copy-paste depending on your system.
The entire loop takes 30–90 seconds after the visit if the AI got it mostly right. If you’re correcting half the note, you’re not saving time—you’re adding steps.
7 Real-World AI Medical Scribe Workflows
1. Primary Care Office Visits
AI scribes shine in routine primary care. Annual physicals, diabetes follow-ups, hypertension checks—these visits follow predictable patterns. The scribe captures chief complaint, reviews systems, documents exam findings, and generates assessment/plan in 20–30 seconds post-visit.
Best fit: chronic disease management, preventive care, same-day sick visits
I’ve seen primary care docs cut 15 minutes per visit by not typing during encounters. More eye contact. Less “hold on while I document this.”
2. Specialist Consults
Specialists deal with longer histories and complex assessments. Cardiology consults can run 45 minutes with extensive medication reconciliation. Orthopedic surgeries need detailed operative planning. AI scribes help organize differential diagnoses and multi-step treatment plans, provided you’ve tuned templates to your specialty.
Best fit: new patient consults, post-op follow-ups, multidisciplinary tumor boards
Generic templates fail here. If your scribe doesn’t understand cardiomyopathy subtypes or ACL reconstruction protocols, you’ll spend more time fixing notes than writing them from scratch.
3. Telehealth and Video Visits
Most AI scribes integrate with Zoom, Microsoft Teams, or telehealth platforms via system audio capture. This eliminates the worst part of virtual care—typing while on camera. The scribe records the video call, generates a note, and syncs it back to your EHR.
Best fit: behavioral health, medication refills, chronic care management, remote follow-ups
Telehealth documentation used to take longer than in-person because you’re juggling three screens. AI scribes fix that.
4. Inpatient Rounds and Consults
Hospitalists and consult services use AI scribes to summarize bedside discussions into daily progress notes. Mobile workflows let you review and sign notes between patients instead of batching documentation at 8 PM.
Best fit: daily progress notes, consult follow-ups, discharge summaries
The challenge? Hospital environments are noisy. Multiple speakers. Interruptions. If your scribe can’t filter background conversations or identify speakers accurately, you’ll get garbage output.
5. Emergency and Urgent Care
ED and urgent care scribes need low latency. You can’t wait 5 minutes for a note when you’re seeing 25 patients per shift. Some platforms promise real-time draft generation as the visit progresses. This works for lower-acuity fast-track visits. It breaks down for trauma or critical care.
Best fit: fast-track, tele-urgent care, lower-acuity visits
I wouldn’t trust an AI scribe for critical resuscitation documentation. Too much risk of missed details.
6. Inbox, Phone, and Portal Encounters
Some AI scribes extend beyond visits to summarize long patient portal messages or phone calls. You paste the text or upload an audio file, and the scribe drafts a response with billing codes for telephone E/M.
Best fit: patient portal threads, telephone triage, refill requests, lab result discussions
This is underrated. Inbox work eats 30–60 minutes per day for most clinicians. Automating even half of it compounds.
7. Letters, Summaries, and Referrals
AI scribes can repurpose visit notes into referral letters, work excuses, or patient-friendly after-visit summaries. Some platforms auto-generate patient summaries explaining diagnoses and next steps in plain language.
Best fit: specialty referrals, FMLA forms, employer disability paperwork
If you’re spending 10 minutes per referral letter, this feature alone justifies the cost.
Benefits of AI Medical Scribes (With Real Numbers)

Early studies and pilots report:
- 50–70% reduction in documentation time per visit (UC San Diego, Stanford pilots)
- 1–2 hours less after-hours charting per day (Epic UserWeb surveys)
- 15–20% improvement in physician work-life balance scores (Nuance DAX studies)
- More consistent note structure, which helps billing teams, quality reporting, and legal defensibility
The key word is consistent use. Doctors who use AI scribes for every visit see these gains. Doctors who cherry-pick easy visits don’t.
More eye contact with patients is real. I’ve watched clinicians go from staring at a screen 60% of the visit to maintaining eye contact 80% of the time. Patients notice.
Risks, Limitations, and What AI Medical Scribes Cannot Do
AI scribes introduce new failure modes you need to manage:
Hallucinations and Omissions
The AI will generate plausible-sounding text that never happened. “Patient reports excellent adherence to medications” when they actually said they stopped taking metformin last month. Or the scribe omits critical information because it wasn’t phrased clearly.
You catch this during review. If you’re rubber-stamping notes without reading them, you’re creating medico-legal time bombs.
Misattribution
AI scribes struggle with multi-speaker environments. They’ll attribute your words to the patient or vice versa. If a family member speaks, the scribe might assign their statements to the patient.
Fix: Use platforms that train on your voice specifically and support speaker diarization.
Over-Documentation
Some AI scribes generate excessively long notes with paragraphs of fluff. This makes it harder for the next clinician to find key information. Long notes also increase audit risk—if you didn’t do a 14-point ROS, don’t sign a note that says you did.
Fix: Aggressively tune templates to match your actual workflow. Delete sections you don’t use.
Technical Failures
Poor audio quality. Network drops. EHR API timeouts. I’ve seen clinics lose entire mornings because the scribe software crashed and no one had a backup plan.
Fix: Have a manual documentation fallback. Don’t schedule 25 patients on the first day you pilot an AI scribe.
AI scribes do not make diagnoses, choose treatments, or replace clinical judgment. They’re documentation tools. Final responsibility rests with the physician signing the note.

HIPAA, Privacy, and Security Considerations
Any AI medical scribe handling PHI must meet strict requirements:
- HIPAA-compliant infrastructure with encryption in transit (TLS 1.3) and at rest (AES-256)
- Signed Business Associate Agreement (BAA) between your practice and the vendor
- Data residency and retention controls—know where audio and notes are stored and for how long
- Access controls and audit logs—you need to see who accessed patient data and when
- Clear data use policies—will your data train future AI models? Can you opt out?
Some platforms delete audio after note generation. Others retain it for 30–90 days. Know your vendor’s policy.
Patient consent: Most practices inform patients via signage or verbal notification. Some include language in consent forms. There’s no federal requirement for explicit consent, but state laws vary. Check your jurisdiction.
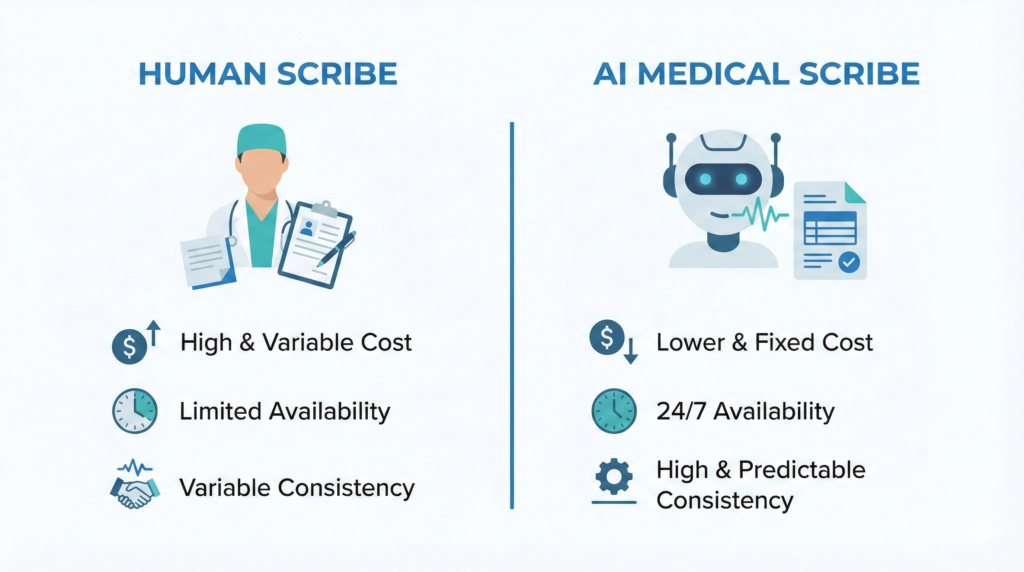
AI Medical Scribe vs Human Scribe: 2026 Comparison
| Factor | AI Scribe | Human Scribe |
|---|---|---|
| Cost per encounter | $0.50–$3.00 | $15–$30 |
| Availability | 24/7, unlimited clinicians | Limited by staffing |
| Accuracy | 85–95% (depending on audio) | 90–98% (with experienced scribes) |
| Context sensitivity | Struggles with subtle context | Experienced humans excel here |
| Scalability | Instant scaling across practice | Requires hiring & training |
| EHR integration | API sync, minimal manual work | Manual typing, EHR interaction |
Hybrid models are winning in 2026. Use AI for routine visits. Deploy human scribes for complex consults, high-risk procedures, or situations where context sensitivity matters.
I’ve seen large health systems run AI scribes for 80% of visits and keep a pool of human scribes for the remaining 20%. This balances cost with quality.
How to Choose an AI Medical Scribe for Your Practice
Use this checklist when evaluating vendors:
Clinical Fit
- Does it support your specialty? (Primary care templates differ from cardiology or orthopedics)
- Can you customize note style, templates, and sections?
- Does it handle multi-problem visits or only single-issue encounters?
Workflow Integration
- How does it connect to your EHR? (Native Epic integration vs manual copy-paste)
- Is review/editing fast enough during clinic flow?
- Can you sign notes within the scribe platform or must you export to EHR first?
Accuracy and Reliability
- What benchmarks or studies has the vendor published?
- How often do pilot users need major corrections?
- Does accuracy degrade with accents, background noise, or fast speech?
Security and Compliance
- Is there a signed BAA with clear PHI policies?
- Are data storage, access, and retention policies transparent?
- Can you audit who accessed patient data?
Burnout and Satisfaction Impact
- Do pilot users report less after-hours charting?
- Does it actually feel like less work, not more cognitive load?
- What’s the Net Promoter Score from current users?
Support and Onboarding
- Is training available for AI medical scribe for clinicians and staff?
- How quickly can issues be resolved for AI medical scribe? (24/7 support or business hours only?)
- What’s the vendor’s roadmap for new features for AI medical scribe?
Run a 4–8 week pilot for AI medical scribe with 5–10 clinicians. Measure documentation time, after-hours work, and satisfaction before and after. Don’t scale until you’ve validated ROI.
Getting Started with AI Medical Scribes in 2026
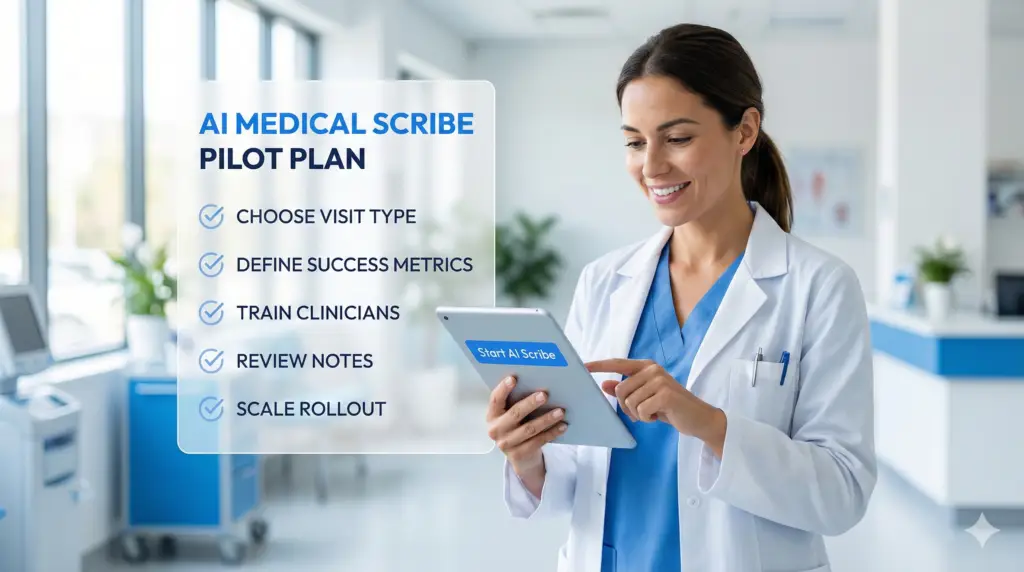
If you’re curious but skeptical, take a staged approach:
Week 1–2: Start with low-risk visit types—follow-ups, telehealth, or preventive care where templates are predictable.
Week 3–4: Limit to a small pilot group of clinicians who are open to experimenting and giving detailed feedback.
Week 5–6: Measure the basics—documentation time, after-hours work, physician satisfaction, and any patient feedback.
Week 7–8: Iterate templates and workflows based on pilot data. Fix broken integrations. Train stragglers.
Don’t scale before you’ve validated that review takes less time than manual documentation. If clinicians are spending 5 minutes fixing AI hallucinations, you’ve failed.
Used thoughtfully, AI medical scribes shift documentation from a nightly burden to a background task. But “thoughtfully” is doing a lot of work in that sentence. Pilot carefully. Measure obsessively. And never sign a note you haven’t actually read.
Pingback: AI Scribe for Doctors: Proven Ways to Reduce Charting Time and Prevent Burnout in 2026